
Previous articles:
Indonesia’s National Transportation Safety Commission today released its final report on the Merpati MA-60 (PK-MZK) accident in Kaimana that occured a year ago, on 7 May 2011. Little has changed on the causes of the accident since the preliminary release made just under a year ago. Controversy surrounding the aircraft airworthiness is not under question as the probably causes of the accident reveals to be more human, and eerily familiar… that is, conducting a visual approach under instrument meteorological conditions.
The accident flight ended with the aircraft hitting the water 800 meters to the south-west of the beginning of runway 01, after a failed go-around attempt, killing all 25 on board. The crew had attempted to conduct an approach into Kaimana’s Utarom airport, amidst rain conditions with a 2 kilometer visibility and 1400ft cloud base. Unfortunately, the airport has no instrument approaches and any approaches are to be made visually, requiring visibility of 5 kilometers or better. Instead of holding or diverting, the crew continued to attempt the approach.
The final sequence summary:
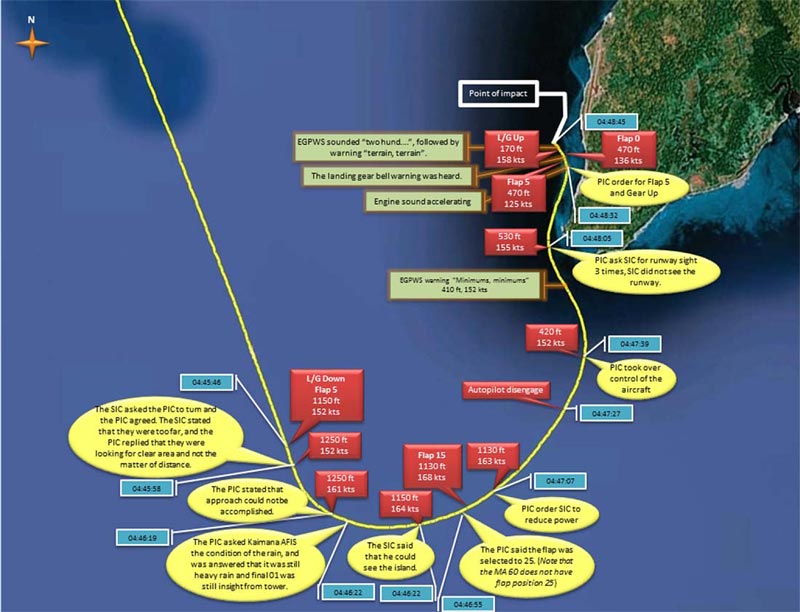 |
| Finale sequence of PK-MZK (Source: NTSC) |
The aircraft impacted the water 800 meters from the runway, broke into 5 large pieces and debris was strewn across a 100m by 200m area on the sea floor 7 – 15 meters below the surface. Landing gear lever was found in the up position, flap lever in the up position, and the power levers in the forward position, and the engine condition levers in the maximum forward position.
Late go-around, loss of situational awareness, and breakdown of CRM
The investigation found that no approach briefing was made, and that the crew were preoccupied in finding the runway which lead to reduced situational awareness, amplified by PIC taking over from the SIC without adequate explanation. When the aircraft reached the “minimum” at around 500ft, approach was not immediately aborted and the PIC instead asked the SIC three times whether or not he could see the runway or not, before finally aborting the approach. Instead of aborting at 500ft, the aircraft had gone as low as 376ft before peaking at 585ft and then the subsequent descent to impact.
The investigation found that the disastrous go-around was a “loss of situational awareness due to a strong intention of the crew to find the runway in poor visibility” and exacerbated by the flap retraction to 5 at low speed (below the required 135kts).
Findings and Factors:
- Visual Flight Rules approach in Instrumental Meteorological Conditions should not have been attempted.
- Crew did not conduct approach checklist or conduct approach briefings.
- The lack of approach briefing exacerbated the impending danger of attempting to conduct a visual approach in unsuitable condition because the crew did not synchronize their plan of attack.
- Engine Regime Selector (ERS) was not selected to TOGA during the go-around or in the approach (as required by the approach checklist). This limited the engine Torque to a maximum of 85.6% instead of 106.3% for TOGA.
- Crew lacked situational awareness by trying to find the runway, and then discontinued the approach.
- Crew actions of retracting flaps to 5 then up, less than go-around power, and increased roll up to 38 degrees left bank led to rapid descent impact with water.
- Both crew had low experience on type. Both PIC and SIC had less than 250hrs on type. This situation may have contributed to the accident.
- Evidence indicating steep cockpit authority may have added to the breakdown in crew resource management.
- Inadequate / ineffective training program may have lead to deviations from standard procedures and regression to habits associated with previous aircraft type. The “flaps at 25” and retraction to flap 5 during the go-around also reflect the PIC’s previous type rating, the Fokker 100. This could be exacerbated by lack of training in a new type.
- There was no evidence that the crew had received EGPWS training.
- The FCOM and Aircraft Maintenance Manual used non-standard English Aviation Language. Although this does not directly contribute to the accident, it could have caused confusion.
- Flight Operations Quality Assurance had not been implemented and the airline had not been effective at implementing the Safety Management System in all management levels.
- DFDR (Digital Flight Data Recorder) did not comply with Indonesian CASR 121.343 and 121.344 requirements. It did not record lateral and longitudinal acceleration as required (Chinese Civil Aviation Regulations 121 did not require these two parameters).
Since the accident, the NTSC reported that the DGCA has audited Merpati Airlines, and that the Safety Management System have been implemented at all management levels in Merpati. Merpati itself has issued various internal safety recommendations as a result of this incident.
It’s not the first time for Merpati…
However, as a consumer and member of the general public, I cannot help but wonder, if safety improvements will prevail in Merpati. Afterall, just a year before PK-MZK, a Merpati 737-300 overran the runway at nearby Manokwari, and again, it was conducting a visual approach in instrument meteorological conditions, just like in Kaimana. That 737-300, PK-MDE, though had no fatalities, was written off after that spectacular accident!
Sources:
All sources can also be found at NTSC original site.
pilot was too experienced to conduct normal procedures?